Tonsil stones, also known as tonsilloliths, are mineralizations of debris within the crevices of the tonsils.[1][3] When not mineralized, the presence of debris is known as chronic caseous tonsillitis (CCT).[1] Symptoms may include bad breath,[1] foreign body sensation, sore throat, pain or discomfort with swallowing, and cough.[4] Generally there is no pain, though there may be the feeling of something present.[1] The presence of tonsil stones may be otherwise undetectable; however, some people have reported seeing white material in the rear of their throat.
| Tonsil stones | |
|---|---|
| Other names | Tonsillolith, tonsillolithiasis, tonsillar stones, chronic caseous tonsillitis |
 | |
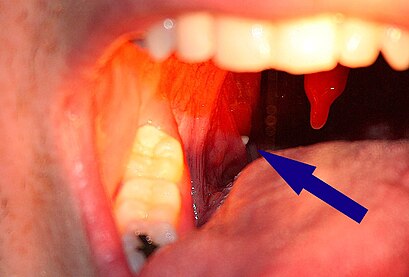
| A tonsillolith lodged in the tonsillar crypt | |
| Specialty | Otorhinolaryngology |
| Symptoms | Discomfort, bad breath[1] |
| Risk factors | Recurrent throat infections[2] |
| Differential diagnosis | Calcified granulomatous disease, mycosis, syphilis[2] |
| Treatment | Gargling with salt water, tonsillectomy[1] |
| Medication | Chlorhexidine or cetylpyridinium chloride[1] |
| Frequency | Up to 10%[1] |
Risk factors may include recurrent throat infections.[2] Tonsil stones contain a biofilm composed of a number of different bacteria, and calcium salts, either alone or in combination with other mineral salts.[5][1] While they most commonly occur in the palatine tonsils, they may also occur in the adenoids, lingual tonsils and tubal tonsil.[3][6][7] Tonsil stones have been recorded weighing from 0.3 g to 42 g,[3] and they are typically small in size. However, there are occasional reports of large tonsilloliths. They are often discovered during medical imaging for other reasons and more recently, due to the impact and influence of social media platforms such as TikTok, medical professionals have experienced an increase in patient concern and tonsillolith evaluations.[8][9]
They are usually benign, so if tonsil stones do not bother the patient, no treatment is needed.[1] However in rare cases, tonsilloliths have presented patients with further complications necessitating surgical extraction. Tonsilloliths that exceed the average size are typically seen in older individuals as the likelihood of developing tonsil stones is linear. Otherwise, gargling salt water and manual removal may be tried.[1] Chlorhexidine or cetylpyridinium chloride may also be tried.[1] Surgical treatment may include partial or complete tonsil removal.[1][10] Up to 10% of people have tonsil stones.[1] Biological sex does not influence the chance of having tonsil stones,[1] but older people are more commonly affected.[2] Many people opt to extract their own tonsil stones manually or with developments in dental hygiene products. Water flossers have become a more common mechanism to extract tonsilloliths and alleviate the discomfort and complications they exacerbate. Tonsil stones can become dislodged on their own while eating, drinking, gargling, and coughing. Additionally, an exhalation technique that vigorously shakes the tonsils may be performed to dislodge them. This involves loudly producing a voiceless velar fricative sound, at various pitches to shake both the palatine and lingual tonsils.
Signs and symptoms
editTonsil stones may produce no symptoms or they may be associated with bad breath.[1] In fact, many dental professionals argue that tonsil stones are the leading cause of bad breath in their patients. The smell may be that of rotting eggs.[11] Tonsil stones tend to happen most often in people with longterm inflammation in their tonsils.[12]
Occasionally there may be pain when swallowing.[13] Even when they are large, some tonsil stones are only discovered incidentally on X-rays or CAT scans. Other symptoms include a metallic taste, throat closing or tightening, coughing fits, itchy throat, and choking.
Larger tonsil stones may cause recurrent bad breath, which frequently accompanies a tonsil infection, sore throat, white debris, a bad taste in the back of the throat, difficulty swallowing, ear ache, and tonsil swelling.[12] A medical study conducted in 2007 found an association between tonsilloliths and bad breath in patients with a certain type of recurrent tonsillitis. Among those with bad breath, 75% of the subjects had tonsilloliths, while only 6% of subjects with normal halitometry values (normal breath) had tonsilloliths. A foreign body sensation may also exist in the back of the throat. The condition may also be an asymptomatic condition, with detection upon palpating a hard intratonsillar or submucosal mass.
-
 A tonsillolith protrudes from the tonsil
A tonsillolith protrudes from the tonsil -
 Large tonsillolith half exposed on tonsil
Large tonsillolith half exposed on tonsil -
 Closeup of a tonsillolith
Closeup of a tonsillolith



Pathophysiology
edit
The mechanism by which these calculi form is subject to debate,[3] though they appear to result from the accumulation of material retained within the crypts, along with the growth of bacteria and fungi—sometimes in association with persistent chronic purulent tonsillitis.
In 2009, an association between biofilms and tonsilloliths was shown. Central to the biofilm concept is the assumption that bacteria form a three dimensional structure, dormant bacteria being in the center to serve as a constant nidus of infection. This impermeable structure renders the biofilm immune to antibiotic treatment. By use of confocal microscopy and microelectrodes, biofilms similar to dental biofilms were shown to be present in the tonsillolith, with oxygen respiration at the outer layer of tonsillolith, denitrification toward the middle layer, and acidification toward the core.[14]
Cause and diagnosis
edit
Diagnosis is usually made upon inspection. Tonsilloliths are difficult to diagnose in the absence of clear manifestations, and often constitute casual findings of routine radiological studies. The cause of tonsil stones can include a multitude of sources from bacterial infections, streptococcus bacteria, viral infections, adenoviruses, influenza virus, enteroviruses and parainfluenza virus.[15]
Classification
editTonsilloliths or tonsil stones are calcifications that form in the crypts of the palatal tonsils. They are also known to form in the throat and on the roof of the mouth. Tonsils are filled with crevices where bacteria and other materials, including dead cells and mucus, can become trapped. When this occurs, the debris can become concentrated in white formations that occur in the pockets.[12] Researchers found aerobic bacteria present on the surface of tonsilloliths and anaerobic bacteria at the core of tonsilloliths. They have the potential to cause oral halitosis as they contain volatile sulfur compounds and sulfur derived gases, foul smelling compounds produced during bacterial metabolism.[16] Tonsilloliths are formed when this trapped debris accumulates and are expressed from the tonsil. They are generally soft, sometimes rubbery. This tends to occur most often in people who suffer from chronic inflammation in their tonsils or repeated bouts of tonsillitis.[12] They are often associated with post-nasal drip.
Enlarged tonsil stones
edit
Much rarer than the typical tonsil stones are giant tonsilloliths. Giant tonsilloliths may often be mistaken for other oral maladies, including peritonsillar abscess, and tumors of the tonsil.[17] On average, tonsil stones should appear within a similar range of the image on the right; however, individuals with extenuating cases have been reported. In these instances, extensive care such as extraction by a licensed medical professional may be needed.
Differential diagnosis
editImaging diagnostic techniques can identify a radiopaque mass that may be mistaken for foreign bodies, displaced teeth or calcified blood vessels. CT scan may reveal nonspecific calcified images in the tonsillar zone. The differential diagnosis must be established with acute and chronic tonsillitis, tonsillar hypertrophy, peritonsillar abscesses, foreign bodies, phlebolites, ectopic bone or cartilage, lymph nodes, granulomatous lesions or calcification of the stylohyoid ligament in the context of Eagle syndrome (elongated styloid process).[18]
Differential diagnosis of tonsilloliths includes foreign body, calcified granuloma, malignancy, an enlarged temporal styloid process or rarely, isolated bone which is usually derived from embryonic rests originating from the branchial arches.[19]
Treatment
editIf tonsil stones do not bother a person, no treatment is needed.[1] Otherwise gargling saltwater and manual removal may be tried.[1] Chlorhexidine or cetylpyridinium chloride may also be tried.[1] Surgical treatment may include partial or complete tonsil removal.[1]
Some people are able to remove tonsil stones using a cotton swab. Oral irrigators are also effective. Most electric oral irrigators are unsuitable for tonsil stone removal because they are too powerful and are likely to cause discomfort and rupture the tonsils, which could result in further complications such as infection. Irrigators that connect directly to the sink tap via a threaded attachment or otherwise are suitable for tonsil stone removal and everyday washing of the tonsils because they can jet water at low-pressure levels that the user can adjust by simply manipulating the sink tap, allowing for a continuous range of pressures to suit each user's requirements.[12]
There are also manually pressurized tonsil stone removers. A manual pump-type tonsil stone remover can adjust the water pressure depending on the number of pumps, effectively removing tonsil stones.
More simply still, gargling with warm, salty water may help alleviate the discomfort of tonsillitis, which often accompanies tonsil stones. Vigorous gargling each morning can also keep the tonsil crypts clear of all but the most persistent tonsilloliths.[12]
Curettage
editLarger tonsil stones may require removal by curettage (scooping) or otherwise, although thorough irrigation will still be required afterward to effectively wash out smaller pieces. Larger lesions may require local excision, although these treatments may not completely help the bad breath issues that are often associated with this condition.
Laser
editAnother option is to decrease the surface area (crypts, crevices, etc.) of the tonsils via laser resurfacing. The procedure is called a laser cryptolysis. It can be performed using a local anesthetic. A scanned carbon dioxide laser selectively vaporizes and smooths the surface of the tonsils. This technique flattens the edges of the crypts and crevices that collect the debris, preventing trapped material from forming stones.
Surgery
editTonsillectomy may be indicated if bad breath due to tonsillar stones persists despite other measures.[20]
Epidemiology
editTonsilloliths or tonsillar concretions occur in up to 10% of the population, frequently due to episodes of tonsillitis.[21] While small concretions in the tonsils are common, true stones are less so.[3] They commonly occur in young adults and are rare in children.[3]
References
edit- ^ a b c d e f g h i j k l m n o p q r s t Ferguson M, Aydin M, Mickel J (October 2014). "Halitosis and the tonsils: a review of management". Otolaryngology–Head and Neck Surgery. 151 (4): 567–74. doi:10.1177/0194599814544881. PMID 25096359. S2CID 39801742.
- ^ a b c d White SC, Pharoah MJ (2014). Oral Radiology - E-Book: Principles and Interpretation. Elsevier Health Sciences. p. 527. ISBN 978-0-323-09634-8.
- ^ a b c d e f Ram S, Siar CH, Ismail SM, Prepageran N (July 2004). "Pseudo bilateral tonsilloliths: a case report and review of the literature". Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 98 (1): 110–4. doi:10.1016/j.tripleo.2003.11.015. PMID 15243480.
- ^ Bhasme A, Lamba P, Sajjan U (April 2023). "A Case Report of Tonsillolith Treated With Individualized Homoeopathy". Alternative Therapies in Health and Medicine. 29 (3): 88–91. ISSN 1078-6791. PMID 35839105.
- ^ Silvestre-Donat FJ, Pla-Mocholi A, Estelles-Ferriol E, Martinez-Mihi V (2005). "Giant tonsillolith: report of a case". Medicina Oral, Patologia Oral y Cirugia Bucal. 10 (3): 239–242. ISSN 1698-6946. PMID 15876967.
- ^ Leonard JA, Reilly BK (2 February 2022). "Adenoid stones, an unknown culprit in pediatric throat pain". Ear, Nose & Throat Journal. doi:10.1177/01455613221074139. PMID 35107383.
- ^ Bayramov N, Usdat Ozturk A, Ercalik Yalcinkaya S (27 May 2022). "Incidental Soft Tissue Calcifications in Cone-Beam Computed Tomography Images". Turkiye Klinikleri Journal of Dental Sciences. 28 (2): 291–298. doi:10.5336/dentalsci.2021-84346. Retrieved 17 January 2023.
- ^ Sulibhavi A, Isaacson G (26 September 2021). "TikTok Tonsils". Ear, Nose, & Throat Journal. 103 (3): NP183–NP184. doi:10.1177/01455613211038340. ISSN 1942-7522. PMID 34569296.
- ^ Textbook of Oral Radiology. Elsevier India. 2009. p. 607. ISBN 978-81-312-1148-9.
- ^ Wong Chung J, van Benthem P, Blom HM (May 2018). "Tonsillotomy versus tonsillectomy in adults suffering from tonsil-related afflictions: a systematic review". Acta Oto-Laryngologica. 138 (5): 492–501. doi:10.1080/00016489.2017.1412500. PMID 29241412.
- ^ DeVault KR, Wallace MB, Aqel BA, Lindor KD (2016). Practical Gastroenterology and Hepatology Board Review Toolkit. John Wiley & Sons. p. 59. ISBN 978-1-118-82907-3.
- ^ a b c d e f "Tonsil Stones (Tonsilloliths)". WebMD.com. Retrieved 6 March 2016.
- ^ Giudice M, Cristofaro MG, Fava MG, Giudice A (July 2005). "An unusual tonsillolithiasis in a patient with chronic obstructive sialoadenitis". Dentomaxillofac Radiol. 34 (4): 247–50. doi:10.1259/dmfr/19689789. PMID 15961601.
- ^ Stoodley P, Debeer D, Longwell M, Nistico L, Hall-Stoodley L, Wenig B, Krespi YP (September 2009). "Tonsillolith: not just a stone but a living biofilm". Otolaryngology–Head and Neck Surgery. 141 (3): 316–21. doi:10.1016/j.otohns.2009.05.019. PMID 19716006. S2CID 209346548.
- ^ "Should You Worry About Tonsil Stones?: Dr. Raminder Singh: General Dentistry". www.elitedentalanddenture.com. Retrieved 4 May 2023.
- ^ Yellamma Bai K, Vinod Kumar B (July 2015). "Tonsillolith: A polymicrobial biofilm". Medical Journal Armed Forces India. 71 (Suppl 1): S95–S98. doi:10.1016/j.mjafi.2011.12.009. ISSN 0377-1237. PMC 4529540. PMID 26265885.
- ^ Padmanabhan TK, Chandra Dutt GS, Vasudevan DM, Vijayakumar (May–June 1984). "Giant tonsillolith simulating tumour of the tonsil – a case report". Indian J Cancer. 21 (2): 90–1. PMID 6530236.
- ^ Silvestre-Donat F, Pla-Mocholi A, Estelles-Ferriol E, Martinez-Mihi V (2005). "Giant tonsillolith: report of a case" (PDF). Medicina Oral, Patología Oral y Cirugía Bucal. 10 (3): 239–42. PMID 15876967.
- ^ "Images". Archived from the original on 3 December 2012. Retrieved 28 November 2007.
- ^ Darrow DH, Siemens C (August 2002). "Indications for tonsillectomy and adenoidectomy". Laryngoscope. 112 (8 Pt 2 Suppl 100): 6–10. doi:10.1002/lary.5541121404. PMID 12172229. S2CID 24862952.
- ^ S. G. Nour, Mafee, Mahmood F., Valvassori, Galdino E., Galdino E. Valbasson, Minerva Becker (2005). Imaging of the head and neck. Stuttgart: Thieme. p. 716. ISBN 1-58890-009-6.